Androgenetic Alopecia
Androgenetic alopecia (AGA) is defined as inherited hair loss for both men and women that principally is derived from a genetic predisposition to hair loss but that can be affected to varying degrees by other external factors like diet, stress, smoking, and other environmental impacts. Although most commonly associated with men who begin to lose hair at puberty when the effects of dihydrotestosterone (DHT) begin to cause progressive hair loss in them, AGA is highly prevalent in women as well and can strike at any age with a higher incidence in women as they mature, especially in the post-menopausal setting when there can be a predominance of circulating male hormones vis-à-vis female ones.
Male Pattern Baldness
Male pattern baldness, a type of androgenetic alopecia (AGA), is the most common kind of hair loss and the type that comes to mind when we think of hair loss. AGA can affect up to 50% of the male population by age 50 and up to 80% by age 80. Although AGA is clearly inherited genetically, the exact pattern of inheritance is not well defined and is thought to be polygenic in nature, that is, comes from multiple genetic loci, or locations. In fact, only one gene that codes for the androgen receptor has been clearly linked to Androgenetic Alopecia so far. Accordingly, although a family history may be helpful, the expression of hair loss is so variable that it is not always predictive of how you will advance in your hair loss. For example, your father may have a full head of hair, and you may be rapidly balding. Since there are epigenetic influences, that is, environmental effects, that can retard or accelerate hair loss, even genetically identical twins may manifest different degrees of hair loss.
The main hormonal cause of hair loss in men is the presence of dihydrotestosterone (DHT), which is converted from testosterone, on DHT-sensitive scalp hairs (Figure 1), usually in the frontal, crown, and possibly sides of the head in more advanced cases of hair thinning.

Unfortunately, this hair loss is progressive in nature and can be rapidly accelerated by the use of testosterone or ingestion of other supplemental male hormones. Medical therapies, like finasteride and minoxidil (to be discussed below), can be effective in slowing down and restoring miniaturizing (or thinning) hairs on the scalp. For areas of complete baldness, only surgery will be effective by transplanting hairs from DHT-resistant areas like the occipital (back of the head) and beard regions, for example, and moving them into DHT-sensitive zones (Figure 2).


Dr. Norman Orentreich found that DHT-resistant hairs transplanted into DHT-sensitive areas retain their donor characteristics, which has become known as “donor dominance”, which is the principle upon which modern hair surgery is based. The Norwood Scale is an effective tool to describe the various stages of hair loss in men from Norwood 1, no hair loss, to Norwood 7, the most advanced hair loss that resembles a horseshoe shape (Figure 3).

Female Pattern Baldness
Female hair loss is almost as universal as male AGA but remains less recognized as a problem since women lose hair less severely than men do; however, the prevalence of female hair loss is high: 12% of women by age 30, 25% by age 49, and 30% to 40% of women aged 60 to 69 lose hair. Female hair loss is oftentimes a condition that is less talked about and becomes a source of shame for women who think that they are alone in this disease process since they believe erroneously that they are the only ones suffering from this condition. Further, men have the option of shaving their heads but women typically do not. When women lose hair, they can feel a loss of femininity and youth, which can have devastating psychological impacts that may affect them as much or at times more than their male counterparts. Fortunately, the female hormone drive toward hair loss is less powerful than in men, and women rarely become completely bald or as bald as men do. Nevertheless, it is vital to understand the presence and impact AGA has on women.
With women, the problem of hair loss is, however, more complex. There may be hormonal factors that must be evaluated, corrected, or ruled out along with treating the condition possibly both medically and surgically. For example, young women may suffer from low iron due to their menstrual cycle, which can be a leading cause of hair loss. An imbalance of estrogen, testosterone, etc., may be the cause of hair loss, which may benefit from hormone adjustments. In younger women, the condition may be observed in those who have polycystic ovarian disease or in older women in those undergoing menopause. Accordingly, a detailed blood panel should be considered a prerequisite in the workup and evaluation of women with hair loss in addition to a thorough history and physical examination.
For women, medical therapy can be helpful to stabilize and control their disease process like minoxidil and spironolactone. Finasteride, used most commonly in men, must be avoided in women of childbearing age since it can risk birth defects if taken. However, oral finasteride in higher doses has been shown to be effective in postmenopausal women, in whom the benefit is higher and the risk is eliminated. Surgery for AGA in women can help restore their lost vitality and femininity (Figure 4).

Even though women usually have less global hair loss than men, they oftentimes have less donor capacity, that is usable donor hairs to transplant, than men. Effective strategies for women include transplanting areas in a selective fashion to concentrate the results for optimal outcomes. For example, a T, L, or reverse L pattern can be used to focus the transplant on one chosen hair part (right, left or center) – the vertical limb of the T, L, or reverse L – and the central forelock (the center frontal hair loss, a critical zone in most cases) – the horizontal limb of the T, L, or reverse L (Figure 5).

In addition to these patterns, sometimes women need to lower their hairline usually most commonly for one of two reasons: they are born with a high hairline (Figure 6) (which is not AGA) or menopausal hair loss causing loss of the frontal hairline frame (Figure 7) like in men.


There are other conditions like traction alopecia caused by tight braiding, more commonly occurring in Black women, which mimics AGA (Figure 8).

There are many scales to define female hair loss but the most commonly used one is the Ludwig scale which defines mild (Ludwig 1), moderate (Ludwig 2), and severe (Ludwig 3) hair loss (Figure 9).

Hair Growth and Androgenetic Alopecia
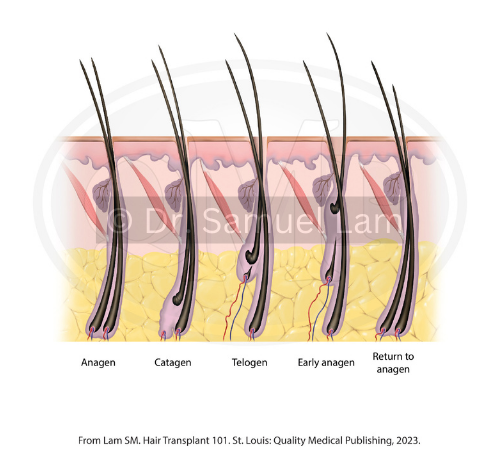
The hair growth cycle is composed of four phases: anagen, catagen, telogen, and exogen (Figure 10). The stage of hair growth begins with the anagen phase, which is the longest phase lasting about 2 to 6 years. The catagen phase starts when the anagen ends and lasts about 1 to 2 weeks. During this phase, hairs stop driving new cellular growth. The telogen phase lasts about 3 to 5 months, and an estimated 10% of scalp hairs are in this phase. It is at the beginning of the exogen phase that newly formed hairs start to wake up while the old hairs are pushed out. This phase lasts about 2 to 5 months, during which time, hairs are shed from the scalp, often helped by washing and brushing. In AGA, anagen growth cycles can shorten from 4 to 6 years to 1 year or less with an increase in the percentage of telogen hairs.
In addition to the above shortening of anagen and an increase in telogen hairs, the principal method of hair loss in AGA involves the gradual progression of thick “terminal” hairs into thin, short, and semi-transparent hairs known as miniaturized or vellus-like/vellus hairs. These vellus hairs eventually disappear and lead to a completely bald appearance. What is interesting is that there is still a hair follicle below the skin even in a completely slick bald scalp. As mentioned, dihydrotestosterone (DHT)-sensitive hair follicles undergo this process of miniaturization and eventual baldness by virtue of the effects of DHT on these scalp hairs. DHT can be minimized by blocking the enzyme 5-alpha-reductase that converts testosterone to DHT. That is how finasteride works by blocking the main enzyme 5-alpha-reductase type 2, which is in charge of about 69% of circulating DHT, whereas dutasteride, another more potent medication, blocks both types 1 and 2 5-alpha-reductase leading to an almost complete (but not total) blockade of this conversion. These medications can slow down the conversion of terminal hairs into vellus hairs and also bring back a portion of vellus hairs into thicker terminal hairs. When true baldness sets in, the effect of these medications is greatly diminished if not altogether useless. However, even in areas of complete baldness, these medications can help limit further progression in other areas of hair loss where complete baldness has not entirely set in.
Symptoms
- Although hair shedding can be part of AGA, in general, AGA usually shows simply progressive hair thinning with the conversion of terminal hairs into vellus hairs in areas of DHT sensitivity, as shown in Norwood and Ludwig pattern diagrams.
- Hair loss is typically painless, where if there are accompanying signs of pain, irritation, or redness, then other non-AGA types of hair loss may be present such as a scarring hair loss, which would require early dermatologist evaluation and treatment.
- Losing about 100-150 hairs a day should be considered normal on days that you shower.
- Abnormal hair breakage may be caused by malnutrition or chemotherapy agents and is usually not a feature of Androgenetic Alopecia.
- Major hair shedding, which may be a presentation of telogen effluvium and not a part of Androgenetic Alopecia, may be caused by recent general anesthesia, major weight loss, especially with protein malnutrition, stress, or significant illness.
- Androgenetic Alopecia may be confused with other forms of hair loss or may be present with other types of hair loss. For example, someone may have a type of scarring hair loss in the frontal scalp known as frontal fibrosing alopecia (FFA) but also be experiencing AGA behind that hairline.
When to see a doctor?
It is important that these general principles outlined in this hopefully informative document not serve to replace the guidance and relationship with a qualified physician specializing in hair loss conditions. In cases of scarring hair loss, a physician who deals with hair loss will usually be able to easily recognize this condition and confirm it with a biopsy, only as necessary, since this type of condition if left unchecked can lead to profound hair loss that cannot be reversed. In cases of Androgenetic Alopecia, it is important to seek a consultation with a physician early on because medical therapy is far more effective in early cases of hair loss before full baldness sets in. The relationship must be established with both a qualified and ethical physician, not a salesman trying to sell you surgery. For example, transplanting young men, especially without medical therapy to slow down hair loss, may lead to future disasters that cannot be fixed. In general, men have progressively increasing demand for hair loss, that is, the area gets bigger and bigger, in the face of ever-decreasing donor supply due to baldness encroaching on that area and also using that donor for surgery. You do not want to be in a situation where you run out of donor hair because you will have an unfixable, unnatural result. Remember that no hair loss surgery is scarless, neither FUE nor FUT, and you will be unable to shave your head. In summary, you should see a physician as early as you can with your hair loss condition to help diagnose and treat the condition before it becomes severe, and you must seek the advice of an ethical physician who is giving you experienced advice and who understands the risk that hair surgery has, especially in young men.
For a consultation with a hair restoration surgeon, access our Find A Doctor tool where you can search for an ISHRS member by location.
Causes
- AGA is caused principally by genetic causes but is usually diagnosed by a thorough history and physical examination.
- As mentioned, despite genetics being the principal reason for AGA, it is important to provide supportive care for the individual suffering from AGA by optimizing one’s lifestyle by abstaining from factors that cause risk like smoking (which has shown to have a direct link in worsening AGA), poor diet, stress, etc.
Diagnosis
- AGA is usually diagnosed by a thorough history and physical examination.
- When suspicious of scarring hair loss or other dermatologic conditions, referral to a dermatologist and possibly a biopsy can be helpful to rule out these conditions.
- For women, a complete blood work evaluating iron, thyroid function tests, and hormones (estrogen, progesterone, testosterone, dehydroepiandrosterone sulfate [DHEAS]) can be very helpful if not important as part of the initial workup.
Treatment
The general classification of treatment options includes biochemical and natural therapies. Biochemical therapies usually modify DHT directly or indirectly like finasteride and dutasteride but also include minoxidil which does not have as clear a mechanism of how this medication grows hair. For women, spironolactone is also sometimes used and may be part of a regimen to control hair loss. In terms of natural therapies, there are many types, including topical, oral (pills), injections (platelet-rich plasma, etc.), and many other types of therapies. These treatments do not use prescription-based medicines but instead rely on vitamins, growth factors, laser light, etc. Although many believe that only prescription therapies work, there has been a growing body of evidence to support the validity of these natural products as standalone treatments and also combined with biochemical options.
Medications
As mentioned, there are many types of medical therapies, both biochemical and natural, that have been shown to have excellent results. There are only two FDA-approved medical therapies for use for AGA hair loss: oral finasteride for men and topical minoxidil for men and women. It is important to emphasize that a biochemical therapy must be FDA-approved for use in the United States to be used legally in individuals but it only needs to be FDA-cleared for use in the human body. For example, dutasteride, which has been shown to be highly effective in treating male AGA, is FDA-cleared to be used for prostate issues but is used successfully “off-label” (that is, there is no FDA-approved use for hair loss in the US), which is legal but just cannot be advertised by the company manufacturing it for that purpose. Further, 1 mg oral finasteride, which is FDA-cleared for male AGA, has been shown to be effective in post-menopausal women at higher doses of 2.5 and 5 mg but that would also be considered an off-label indication. Finally, these same FDA-cleared medications may be delivered through different routes, for example, topical finasteride and oral minoxidil, which again would not fall under strict FDA-approved indications and be considered off-label usage. This website will navigate these medications in separate pages in even greater detail with this page giving only an overview of the medications for use.
Minoxidil
The FDA-approved method of delivery for minoxidil for androgenetic alopecia is only topical (Figure 11). However, recently, oral minoxidil (Figure 12) has surged in popularity, offering a method of delivery that may have higher efficacy and easier compliance than topical administration. Initially, the FDA cleared minoxidil at 5% for men and 2% for women twice daily, but as of 2014, the FDA has cleared the 5% dose for women once daily. In general, many individuals use these medications at either concentration once daily, with already excellent results.


Although oral minoxidil requires a prescription, topical minoxidil in both 5% and 2% concentrations has been over-the-counter (OTC) since 1996. It is unclear exactly how minoxidil works since it does not regulate androgen hormone, unlike finasteride, but may work to improve hair growth through other methods, for example, lengthening the anagen hair-growth phase. The goal of minoxidil is to adequately place the product on the scalp, not the hair, where it will most effectively work. It may cause temporary hair shedding in the first few weeks to months, which only signifies that hairs are moving out of telogen into the anagen phase, and you should not be alarmed.
Minoxidil has been known to have some adverse side effects like dermatitis and scalp irritation, and, for women, it can cause unwanted hair growth in other parts of the face or body, not due to spillage but systemic (body/bloodstream) absorption. Even though results may become apparent as early as 6 to 12 weeks, it really takes 6 to 12 months to truly see optimal results from therapy. Unfortunately, like with all medications, when stopped over a few months’ time, all the gains achieved will dissipate, and you will return to the state of hair loss you would have been in if you had never used the medication.
Oral minoxidil may bypass some of the limitations of topical minoxidil in that it does not require activation in the scalp skin of minoxidil into its active metabolite, minoxidil sulfate, which can be diminished in some individuals’ scalps. However, oral minoxidil may have more potent adverse events, like lower blood pressure, heart palpitations (feeling the heart beat too fast), swelling in the legs, or more facial/body hair growth, than topical administration.
Only a consultation and monitoring by a qualified physician will help you decide what is suitable for you. Finally, a question asked is whether using minoxidil and finasteride together is necessary in men to combat Androgenetic Alopecia, and the answer is that the two together synergistically combine to achieve greater results than either treatment alone.
Finasteride
Finasteride, marketed under the brand name Propecia by Merck, has been FDA-cleared for male AGA since 1997 at a 1 mg dose and since 1992 at a 5 mg dose to treat benign prostatic hyperplasia. Since 2013, Merck has lost its patent for Propecia, and generic versions of its oral medication can now be obtained without the need to cut a 5 mg pill that was more common practice prior to that time to save on medication costs.
Finasteride is a 5-alpha-reductase type 2 inhibitor that blocks the enzymatic conversion of testosterone to dihydrotestosterone (DHT), which, as stated, is the major cause of male AGA. This medication can block approximately 69% of circulating DHT with effective slowing down of AGA and thickening of miniaturizing hair follicles from AGA. Finasteride cannot be safely used in women who are pregnant due to the risk of birth defects, specifically a hypospadias defect in a male fetus, and men who ingest the pill who are around a pregnant woman should caution their female partner’s inadvertent ingestion of a pill for that reason.
Sexual Side-Effects
Unfortunately, finasteride has been shrouded in a legacy of fear and disinformation since the Journal of Sexual Medicine first reported claims in 2011 and 2012 of what has become known as “post-finasteride syndrome” which means the persistence of sexual side effects despite stopping medication for at least 3 months prior. These reports by the journal were only reflective of unstructured telephone calls and were not reflective of a controlled study. Even though persistent side effects are most likely quite uncommon, it is important to discuss this with a patient considering this therapy. Although Merck’s initial trials showed a very low rate of sexual side effects (below 1%), there was also a study that showed that men given the 5 mg dose (for prostate issues) being counseled that they could have a sexual side effect with finasteride experienced a sexual side effect in 43.6% of cases, whereas those not counseled on the potential of a sexual side effect had a 15.3% chance of experiencing one.
In 2005, the Prostate Cancer Prevention Trial (PCPT) found that the 5 mg dose could lower the risk of prostate cancer by 25%, but it seemed to be associated with higher-grade tumors. The 2008 PCPT update showed that the reason for the results found in the 2005 study may have arisen from the reduced prostate size and thereby reflected a higher detection rate rather than a higher cancer rate. A 2013 PCPT follow-up report found no increase in mortality from prostate cancer in those who took finasteride.
Due to perceived systemic risks with oral finasteride, there has been an increasing trend to favor topical finasteride as an alternative that may offer similar benefits with reduced risk. Topical finasteride comes in different formulations, most commonly in 0.1% and 0.25%, and can be combined with topical minoxidil along with other ingredients as a single treatment option. A randomized, double-blind, controlled study evaluated 0.25% finasteride mixed with 3% minoxidil versus 3% minoxidil alone in the treatment of Androgenetic Alopecia in men aged 18 to 60 and found at week 24 that the combined solution offered a statistically significant improvement over minoxidil alone by studying hair density, hair diameter, and global photographic assessment (p <0.05). The study also found that the combined solution had only a negligible reduction in serum DHT of approximately 5%.
Finasteride, whether topical (Figure 13) or oral (Figure 14), is a first-line defense against male androgenetic alopecia, and despite some controversies, it has been used safely. As of 2012, 20.5 million patient years of therapy have been undertaken for the 5 mg dose and 6.7 million patient years, for the 1 mg dose, with a very low side-effect profile. When combined with minoxidil, these two therapies can be the two most important methods to help reverse and slow down AGA and should be seriously considered after meeting with a hair-loss specialist. Of note, both minoxidil and finasteride have package inserts that discuss the FDA-indication for crown hair thinning. Despite the initial clinical trials aimed at only evaluating the benefits in the crown, both medications have proven successful and important for all areas of the scalp affected by AGA hair loss.


Surgery
There are two major types of surgery to restore hair loss caused by Androgenetic Alopecia: FUE and FUT. FUE is a type of harvesting requiring the removal of hair grafts through a tiny punch from the back of the head, whereas FUT requires a linear incision from the back of the head, which is closed, and the grafts are then dissected from the strip. Both methods only represent harvesting techniques, and a detailed discussion about the pros and cons of each should be explored on their respective pages also found on this website. The other half of the surgical procedure involves making recipient sites into which grafts will then be placed. Over a few months to a year, these transplanted grafts will grow. It is important to emphasize again that FUE and FUT only represent methods of harvesting hairs and not how transplanted hairs are designed or implanted for growth.
As has been mentioned throughout, medical therapy and surgery oftentimes go hand in hand since medical therapy helps slow down hair loss and restore a portion of hairs that are undergoing ongoing thinning, whereas surgery puts hairs where there are none anymore, that is, in areas that are completely bald. For example, if someone is showing thinning in the crown but has completely lost the frontal half of the scalp where there is no more hairline, medical therapy can be used to restore the crown and surgery can be used to restore the entirely lost hairline.
No surgery is scarless despite online marketing to the contrary. FUE leaves tiny lighter-colored dots on the back of the head, and FUT leaves a line on the back of the head. These are not an issue unless the scalp is entirely shaved, so once a hair transplant is performed whether it is FUE (Figure 15) or FUT (Figure 16), you will be unable to shave your head. Further, the grafts that are transplanted are in most cases permanent, so if there is further hair loss that occurs, then additional transplants will be needed to fix any gaps that may appear between the transplanted hairs and the ongoing areas of recession. That is another major reason why medical therapy can be so important to control the progression of hair loss and to minimize the risk of running out of donor hair. The problem as we get older is that we have an ongoing increase in the demand for hair loss with an ongoing decrease in donor supply for either surgery. The goal is to never run out of donor hair or the result will appear unnatural and be unfixable. That is why transplanting hair in younger men, especially without medical therapy, can be dangerous. It is important to meet with an ethical and experienced physician, not a salesman or an unethical surgeon trying to sell you a surgery. Proper consultation to evaluate relative safety for a prospective patient is always a critical first step to minimize taking unnecessary risks in patients.




Platelet-Rich Plasma Therapy
Platelet-rich plasma (PRP) therapy involves taking concentrated growth factors from extracted blood and re-injecting them back into the scalp to help grow hairs non-surgically. There are many protocols of how often to perform the procedure as well as different machines used to purify and concentrate the growth factors. There is no consensus on exactly what is the ideal concentration, which machine performs the best extraction, as well as how much and how often the injection should be performed to achieve results and to maintain those results (Figure 17). PRP can also be undertaken during a hair transplant procedure to further enhance the growth and survival of transplanted grafts.

Low-Level Laser Therapy
Low-level laser therapy (LLLT) provides another natural method of hair restoration for those suffering from Androgenetic Alopecia. LLLT works by photostimulation of the hair follicle by cold laser light in the visible red spectrum using wavelengths between 630 to 670 nm with low power (wattage). Originally, larger office-based units required patients to drive to the office to undergo treatments several times a week but now portable home units, typically either a comb or a helmet design, allow the freedom to undertake these treatments without the effort of a commute. Protocols and designs vary with the disputed benefit of one protocol or device over another.
Upcoming Treatments
There are many innovative treatments for AGA and that landscape is constantly evolving. Some treatments are too new to report or advocate a particular brand or device, which lies beyond the scope and interest of this overview page. Some new treatments include injectable dutasteride into the scalp, which has been shown to be effective and to limit the overall risk of absorption of medicine in the body, thereby reducing the risk of side effects. It is too early to state whether this route of therapy would be an acceptable alternative to traditional oral and topical therapy in terms of long-term benefit to the patient. In addition, there are many oral and topical vitamins from many different manufacturers that claim benefits against AGA, as well as devices that push growth factors, etc., through the scalp. The ultimate treatment, which has yet to materialize, is hair cloning, more properly known as tissue engineering, which will allow unlimited donor hair. However, the horizon timeline for that to be achievable is still unclear and may be many years away still.
Prevention and Healthy Hair Practices
Although there is no way to absolutely avoid or limit the disease process of AGA which is mainly controlled by your genetics, a healthy lifestyle can limit or reverse some of the disease process.
Epigenetic factors, that is, environmental influences that impact one’s genes, have been shown to affect hair loss. The most studied example is smoking or nicotine exposure, which has been proven to accelerate AGA hair loss. That being said, even unstudied variables like diet, exercise, stress, etc., most certainly can impact hair health and hair loss.
References
Lam SM. Hair Transplant 101. Quality Medical Publishing. St. Louis, MO. 2023.
Lam SM, Williams KL., eds. Follicular Unit Excision (FUE) (2nd edition). Jaypee Medical Publishers. New Delhi, India. 2022.
Ellis JA, Sinclair R, Harrap SB. Androgenetic alopecia: pathogenesis and potential for therapy. Expert Rev Mol Med 4:1-11, 2002.
Keene S. Long-term planning in hair transplantation. Presented at the 27th World Congress of the International Society of Hair Restoration Surgery, Bangkok, Thailand, November 2019. Also presented at the 6th Latino Americano de FUE Workshop, Cancun, Mexico, February 2020.
Norwood OT. Incidence of female androgenetic alopecia (female pattern alopecia). Dermatol Surg 27:53-54, 2001.ß
Cash TF, Price VH, Savin RC. Psychological effects of androgenetic alopecia on women: comparisons with balding men and with female control subjects. J Am Acad Dermatol 29:568-575, 1993.
Trüeb RM, Régnier A, Rezende HD, et al. Post-finasteride syndrome: an induced delusional disorder with the potential of a mass psychogenic illness? Skin Appendage Disord 5:320-326, 2019.
Trüeb RM, Luu N-NC, Dias MFRG, et al. How to deal with the issues of fertility, malignancies, and the postfinasteride syndrome while prescribing finasteride for male pattern hair loss. Skin Appendage Disord 8:245-248, 2022.
Irwig MS, Kolukula S. Persistent sexual side effects of finasteride for male pattern hair loss. J Sex Med 8:1747-1753, 2011.
Redman MW, Tangen CM, Goodman PJ, et al. Finasteride does not increase the risk of high-grade prostate cancer: a bias-adjusted modeling approach. Cancer Prev Res (Phila) 1:174-181, 2008.
Suchonwanit P, Srisuwanwattana P, Chalermroj N, et al. A randomized, double-blind controlled study of the efficacy and safety of topical solution of 0.25% finasteride admixed with 3% minoxidil vs. 3% minoxidil solution in the treatment of male androgenetic alopecia. J Eur Acad Dermatol Venereol 32:2257-2263, 2018.
Borges do Nascimento IJ, Harries M, Rocha VB, et al. Effect of oral minoxidil for alopecia: systemic review. Int J Trichology 12:147-155, 2020.
Panchaprateep R, Lueangarun S. Efficacy and safety of oral minoxidil 5 mg once daily in the treatment of male patients with androgenetic alopecia: an open-label and global photographic assessment. Dermatol Ther (Heidelb) 10:1345-1357, 2020.
Hu AC, Chapman LW, Mesinkovska NA. The efficacy and use of finasteride in women: a systematic review. Int J Dermatol 58:759-776, 2019.
Iorizzo M, Vincenzi C, Voudouris S, et al. Finasteride treatment of female pattern hair loss. Arch Dermatol 142:298-302, 2006.
Lourith N, Kanlayavattanakul M. Hair loss and herbs for treatment. J Cosmet Dermatol 12:210-222, 2013.
Dhariwala MY, Ravikumar P. An overview of herbal alternatives in androgenetic alopecia. J Cosmet Dermatol 18:966-975, 2019.
Prager N, Bickett K, French N, et al. A randomized, double-blind, placebo-controlled trial to determine the effectiveness of botanically derived inhibitors of 5-alpha-reductase in the treatment of androgenetic alopecia. J Altern Complement Med 8:143-152, 2002.
Jimenez JJ, Wikramanayake TC, Bergfeld W, et al. Efficacy and safety of a low-level laser device in the treatment of male and female pattern hair loss: a multicenter, randomized, sham device-controlled, double-blind study. Am J Clin Dermatol 15:115-127, 2014.
Kim H, Choi JW, Kim JY, et al. Low-level light therapy for androgenetic alopecia: a 24-week, randomized double-blind, sham device-controlled multicenter trial. Dermatol Surg 39:1177-1183, 2013.
Herman A, Herman AP. Topically used herbal products for the treatment of hair loss: preclinical and clinical studies. Arch Dermatol Res 309:595-610, 2017.
Justicz N, Derakhshan A, Chen JX, et al. Platelet-rich plasma for hair restoration. Facial Plast Surg Clin North Am 28:181-187, 2020.
Kemp P. The evolution of the promise of hair cloning: how hair cell cloning will fit into your practice. Hair Transplant Forum Int 32:37-43, 2022. Available at https://doi.org/10.33589/32.2.37.