What is a FUT Hair transplant?
The term FUT stands for “follicular unit transplantation”. FUT involves removing a strip of tissue 0.5 to 1.5 cm in width and from 5 to 30 cm long from the back of the head, which after having been removed, is closed with sutures or staples. The strip of tissue containing hair and surrounding skin is then expertly dissected into individual follicular unit grafts that will then be transplanted back into the balding areas of the scalp. FUT is known for allowing a high number of grafts to be transplanted in a single session, but it leaves a linear scar in the donor area.

Early History
FUT transplant has been a vital part of the history of hair surgery from its early days and is still widely practiced today with benefits that will be explained later. Historically, before we transplanted individual follicular units, hairs were punched out using large 4-mm punches from the back of the scalp and then transplanted back into the scalp. These larger grafts contained 16 to 20 hairs, or 3 to 4 follicular units, and were known as plugs.
Later these larger plugs were cut down into quarter- and half-sized grafts but in an arbitrary way that did not respect the natural follicular unit groupings. FUT surgery – involving a linear strip of tissue taken from the back of the head – really advanced to its modern incarnation in the late 1980s when Bobby Limmer dissected individual follicular units under a stereomicroscope and showed how natural the results were. This became the gold standard for hair surgery until the rise of FUE (follicular unit excision) in the past decade, which has arrived to challenge FUT surgery with FUE now becoming the dominant and most popular way of performing hair surgery.
Terms used for FUT
As mentioned, FUT and FUE are actually transplanting individual follicular unit grafts, so both methods really constitute “FUT”. Led by the efforts of the American Board of Hair Restoration Surgery (ABHRS), academic hair surgeons have strived to come up with a more accurate term for strip harvesting procedures and the consensus by the ABHRS is that linear strip excision (LSE) is the preferred nomenclature. Nevertheless, in the public’s mind, LSE is simply unknown for the most part, so we will continue to refer to strip harvesting procedures as “FUT” in this section despite the fact that it is not the best term to describe this procedure
Another term used for follicular unit transplantation(FUT) is Follicular Unit Strip Surgery(FUSS).
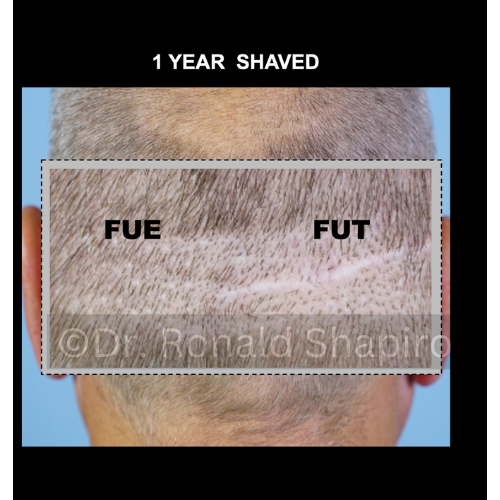
FUT vs. FUE
The two dominant methods today for performing hair transplant surgery are FUE and FUT. FUE involves removing individual follicular units with a micro punch device ranging from 0.7 to 1.2 mm in size (compared with the old punches that were 4 mm in size back in the 1970s). These follicular units are then transplanted back into the balding areas of the scalp.
Also Read: FUE Vs. FUT and Maximizing the Hair Graft Harvest
Unlike FUT, the follicular units aren’t dissected from a single strip but are taken from various parts of the scalp. We’ll discuss the advantages of FUT over FUE in the next section.
Advantages of FUT
FUT offers many distinct advantages over FUE and may be advantageous for certain patients in certain situations. This might not be the case for every patient.
- One major advantage of FUT over FUE is that no shaving is needed.
- FUT also provides the advantage of being able to move a very large number of grafts.
- Faster surgery time as compared to FUE.
- No risk of overharvesting the donor area.
- Cheaper than FUE in most cases.
- Harvested grafts have a lower chance of hair loss as these are taken from the Safe Donor Area(SDA).
Who’s a Good Candidate for FUT?
Who would make the ideal candidate for FUT then? There is no absolutely perfect candidate for one or the other procedure but there may be patients who are more ideally suited for FUT over FUE and vice versa.
Hair Length: One example of an excellent candidate for FUT would be someone who always wears his or her hair longer than an inch and does not want to shave the head to undergo a hair transplant. For example, FUT may be more commonly practiced in women who will never wear their hair super short and will not likely risk ever seeing the scar even if the scar would turn out less than ideal for them. Men who wear their hair very long would also fall into this category.
Age: Older men may also be ideal FUT candidates for several reasons. First, FUT scars heal better with each successive decade in life, that is, a 50 year old would typically have a better FUT scar than a 30 year old individual even though a 30 year old should still heal with a very thin scar if a qualified surgeon performs the procedure.
Hair Loss Stage: Further, individuals with very advanced hair loss, for example, a Norwood 6 or 7, the most advanced hair loss condition, would be better off with an FUT procedure in most cases. The reasons are severalfold. First, the usable donor area is very compressed and narrow, meaning that not many FUE grafts can be harvested without the risk of overharvesting and thinning the donor area. By contrast, oftentimes a lot of FUT grafts can be harvested in many cases from a strip in the center of the narrow donor area. Second, in FUE the grafts would have to be harvested near the border of the hair loss risking graft failure and scar exposure since they are situated beyond the safe donor area (SDA).
These are examples of favorable FUT candidates, but it is vital to have a consultation with an ethical and experienced surgeon to determine whether FUT or FUE would be the ideal procedure for you.
FUT Procedure
In general, the way that the FUT procedure is performed involves certain major steps:
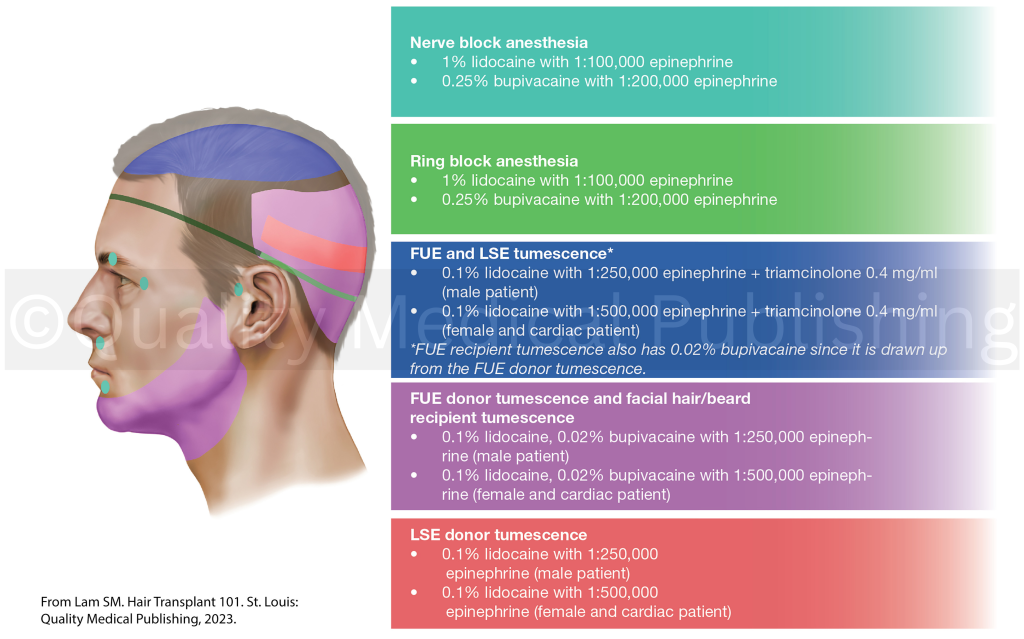
Anesthesia
The first step is to properly anesthetize (numb) the scalp so that surgery can be undertaken. Usually, oral, intramuscular, or intravenous sedation is used at the same time to make the injection of anesthesia more pleasant.
Harvesting and Closure of the Donor Area
Once the anesthetic, which is performed differently by different surgeons, is administered, the surgeon can then remove the strip of tissue from the back of the head without any patient discomfort.
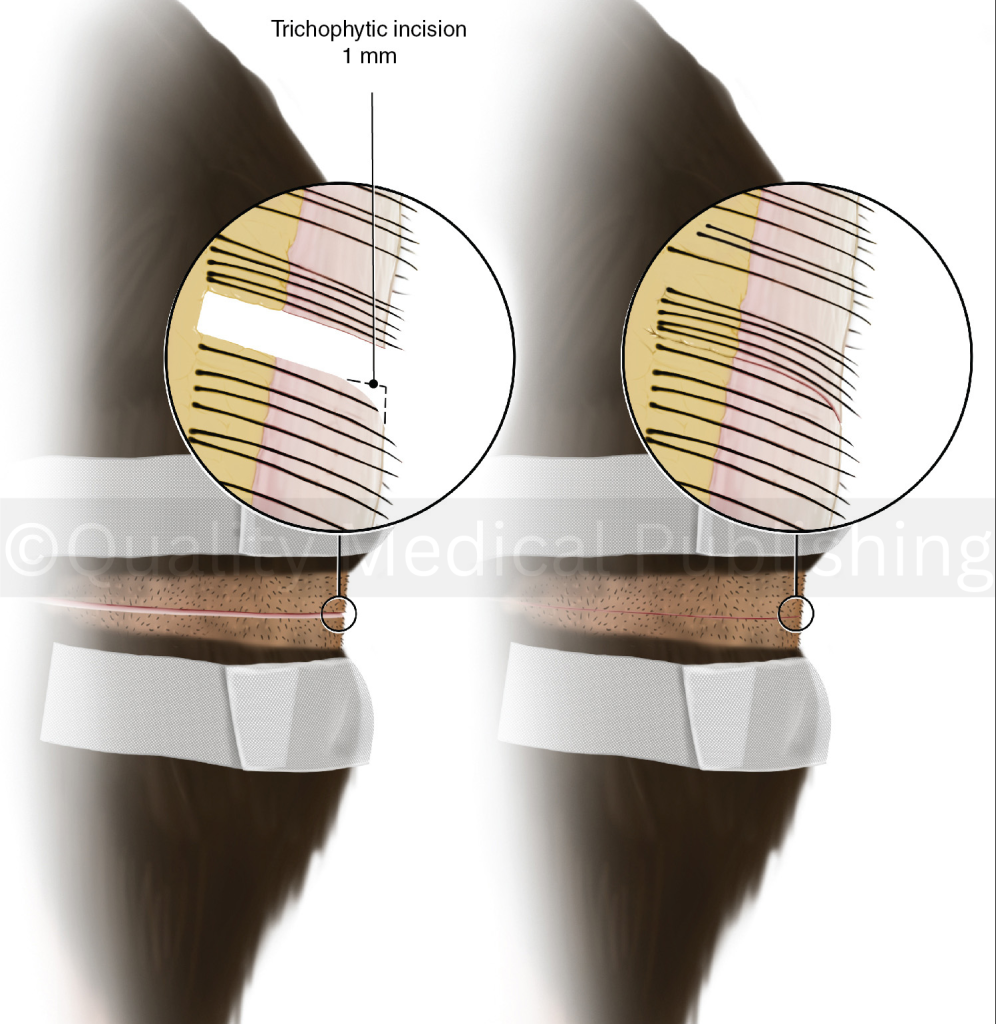
The key to facilitating favorable wound healing in the donor incision is to minimize transection (cutting through hairs and destroying them during harvesting), to avoid damaging nerve and blood supply around the follicles, to close the wound without tension, and to perform a trichophytic incision. The trichophytic incision involves trimming a millimeter of tissue usually from the bottom edge of the wound so that hairs from the bottom edge can grow through the scar, making the incision even more difficult to detect.
Recipient Site Creation
The surgeon then makes recipient sites into which these grafts will be placed.
Graft Dissection
The removed strip is given over to the dissection team that supports the surgeon who then dissects the grafts while the surgeon closes the donor incision using either sutures (stitches) or staples. For graft dissection, the first part of the procedure involves “slivering” in which a row of hairs is dissected free from the strip: think of cutting a slice of bread off of a loaf of bread. This is followed by dissecting the sliver into individual hair follicles divided into 1-, 2-, 3-, and 4-hair grafts.
Graft Placement
The dissected grafts are then finally placed into these sites thereafter, which is usually performed by the dissection team.
FUT Recovery
One advantage described for FUE is that the recovery process is less uncomfortable. In general, that is true. However, with meticulous attention by the surgeon during surgery to avoid irritation and damage to the underlying neurovascular blood supply, usually discomfort levels can be minimized. The nature of recovery differs from surgeon to surgeon and patient to patient.
However, since the donor area is not shaved, that area is entirely hidden during the recovery process from the moment the surgeon is completed unlike in shaved FUE where the donor scabs are visible for about a week afterward.
Use of bandages, sprays, etc., and water and exercise restriction instructions truly differ by the surgeon. You must follow what the surgeon you have chosen recommends for you and not general guidelines posted on this website or even on the websites of other surgeons who have not operated on you.
Accordingly, this section is relatively short to remove any unwanted biases by stating a preferred method of postoperative care or course of recovery.
FUT Side Effects
Side effects following an FUT procedure can be similar but also different from FUE. Some of them are explained below.
Postoperative Pain
With FUT there can be more pain and discomfort than FUE in some cases that usually can be managed with postoperative analgesic medications.
Temporary Hair Loss
Unfortunately, shock hair loss can occur in almost any patient undergoing a hair transplant. Shock hair loss, or telogen effluvium, implies that the native, non-transplanted hairs can undergo temporary shedding making the area involved appear thinner and balder. This more frequently occurs in the recipient area but may also involve the donor area. Most patients are alarmed at this situation but must be reassured that this issue is typically a temporary problem and should be resolved over time. Women are more susceptible to this type of problem and so are men with extensive miniaturization (hairs that are thinning), especially if hairs have not been stabilized preoperatively. For example, medications like minoxidil for women and finasteride and minoxidil for men may help to limit (but not entirely avoid) this risk if taken for at least 6 weeks or longer before the surgery.
Scalp Cysts
There is a very minor risk of infection and scalp cysts that can occur postoperatively that is fortunately usually minor and self-limiting.
Scarring
An unfavorable linear donor scar is obviously what should be avoided but may need to be corrected. There are many ways to correct the scar including the following: re-excision and closure of the scar; transplanting into the scar using either FUE or FUT grafts; and/or scalp micropigmentation (SMP) or tattooing into the scar to either make the scar look closer to natural skin color and/or make tiny pigmented dots to resemble hair follicles.

FUT Hair Transplant Cost
The costs of FUT procedures in general may be less than FUE since the amount of labor on the part of the surgeon is less with FUT than with FUE. That being said, unfortunately, today many patients are offered “cheap” FUE because the surgeon is not actually performing the procedure. Instead, unlicensed technicians are unlawfully performing FUE harvesting, which the ISHRS condemns and which has been described in the ISHRS campaign, Fight the FIGHT. The rise of these “black market” clinics has led to many hair transplant disasters, many of which simply cannot be corrected.
FUT Before and After Pictures
The gentlemen shown had an FUT hair transplant done by Dr. Sam Lam. You can view the before and after results of the hair transplant in 2 different angles.


Choosing the Right Surgeon
Choosing the right surgeon to perform your procedure is the single most important decision for every patient. The surgeon’s reputation is hard won through years of experience and can be evident through word-of-mouth referrals, community reputation, extensive before and after photographs, online reviews, etc.
During your consultation, you will find your level of comfort and rapport with a surgeon who should be the one in charge of your care and devising the strategy to help with your hair loss that may involve medicine alone, surgery alone, or more likely both a combination of medicine and surgery.
If a surgeon has not properly counseled you on medical therapy to combat ongoing hair loss, especially if you are a man, or at least explained how medical therapy would or would not be appropriate for you, then that can be a red flag that the surgeon you are seeking is not ethically and comprehensively evaluating and managing your hair loss condition.
For a consultation with a hair restoration surgeon, access our Find A Doctor tool where you can search for an ISHRS member by location.
References
Lam SM. Hair Transplant 101. Quality Medical Publishing. St. Louis, MO. 2023.
Limmer BL. Elliptical donor stereoscopically assisted micrografting as an approach to further refinement in hair transplantation. J Dermatol Surg Oncol 20:789-793, 1994.
Lam SM. Managing postoperative hair shedding in women. Presented at the 30th Annual Meeting of the International Society of Hair Restoration Surgery, Panama City, Panama, October 2022.
Keene SA, Rassman WR, Harris JA. Determining safe excision limits in FUE: factors that affect, and a simple way to maintain, aesthetic donor density. Hair Transplant Forum Int 28:1-11, 2018.
Unger W, Solish N, Giguère D, et al. Delineating the “safe” donor area for hair transplanting. Am J Cosm Surg 11:239-243, 1994.